

The older a woman is, higher the chance of her losing a pregnancy. The risk starts to increase from mid-30s rapidly.
Although, there are emerging reports to state that a man’s age (if over 40) may also have an indirect effect on conferring an increased risk of miscarriage, one needs to bear in mind that the evidence for this is not strong currently
It is not uncommon to experience a pregnancy loss due to abnormality in the genetic makeup of the pregnancy itself. This does not mean though that you or your partner carry a genetic mutation that can be passed on and result in pregnancy losses, but rather that there has been a problem with the way that the sperm and egg that went into making the pregnancy formed.
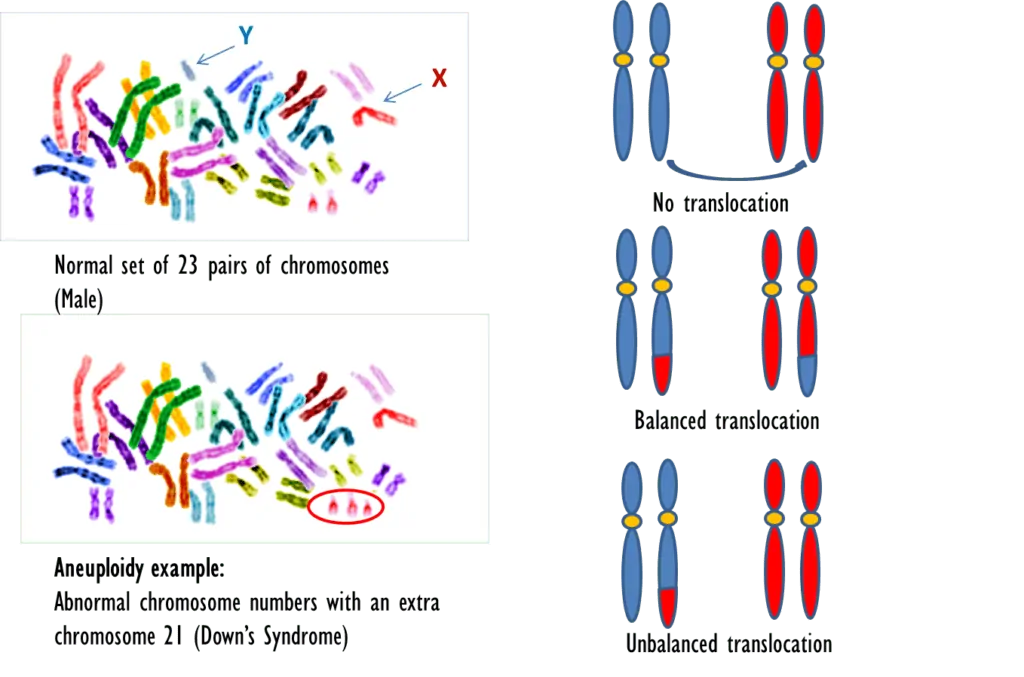
Our DNA is made up of pairs of chromosomes that carry hereditary information in the form of genes. We inherit half of our DNA from our mother and the other half from the father. One of the common chromosome abnormalities that result in a miscarriage is having an extra chromosome. This can be linked to the age of the mother, as the eggs of older women are of lower quality. The older the woman at the time of conceiving, the more likely there is of having a problem with the chromosomes as the dividing egg does not halve the number of chromosomes equally. This in turn results in the embryo either acquiring extra chromosome numbers or having less than the normal set of chromosomes. This type of chromosomal abnormality is collectively referred to as aneuploidy.
Almost half of miscarriages occur due to these types of chromosomal abnormalities of the embryo. This occurs randomly and is not an inherited problem.
However, if on genetic testing it is noted that there is a translocation, meaning that parts of the chromosomes have been swapped around and are now on the wrong chromosomes, places then this may result in recurrent pregnancy loss. This is less common (3-5%). If all genes post cross-over are present, it is known as balanced translocation but if parts of chromosomes are either doubled up or missing altogether, then it would result in what is called an unbalanced translocation. If this is picked up then you and your partner may be offered a genetic testing of your own DNA to see whether you have the genetic condition.
The figure below explains the difference between aneuploidy and translocation type of genetic abnormalities.


At present, strong evidence is lacking that links sperm DNA damage to recurrent early pregnancy loss and most professional bodies do not recommend offering this test.
If all the tests offered to you or your partner have come back clear and there is no known explanation for your pregnancy loss, the doctor would offer you an early pregnancy scan appointment in your future pregnancy. Please also be sure to take folic acid and vitamin D supplements.
Despite having had recurrent early pregnancy losses, it is not all doom and gloom. There is still a high chance of having an ongoing pregnancy and successful live birth.
The prediction chart as shown below by Brigham et al (Human Reproduction, 1999) may be a helpful guide to refer to. The guide is adapted from Brigham et al, Human Reproduction, 1999.

Progesterone therapy: The PROMISE trial (Coomarasamy et al, NEJM, 2015) found that there was no higher chance of having a baby if progesterone was given during early pregnancy, for women who have had recurrent miscarriage. However, a separate study called the PRISM trial (Coomarasamy et al, NEJM, 2019 & AJOG, 2020) did show that a subgroup of women who have had previous EPL and had fresh bleeding in the current pregnancy (threatened miscarriage) may benefit from progesterone supplements. Please discuss this further with your doctor.
Thyroxine use: The TABLET trial (Dhillon-Smith et al, NEJM, 2019) did not show any improvement in chance of having a baby by giving thyroxine tablets to women who had thyroid autoantibodies but who had normal thyroid function. Hence, this is not a recommended treatment if you just have antibodies but do not have a thyroid problem per se.
Immunotherapy: The RESPONSE trial (Eapen et al, Hum Rep, 2019) did not show that women who had suffered from unexplained recurrent miscarriages and were given a synthetic protein (GCF/NT 100) during their early pregnancy, were more likely to have a live birth.
There is no evidence to support role of immunotherapy or steroids for treating recurrent miscarriages.
If you are keen to take part in any research study, your doctor will be the best port of call to give you information about current studies.
Some of the resources listed below are reliable sources of information and hopefully will guide you through this difficult and emotional journey.
- https://www.miscarriageassociation.org.uk/
- https://www.tommys.org/pregnancy-information/pregnancy-complications/baby-loss/miscarriage-information-and-support
- https://www.rcog.org.uk/globalassets/documents/patients/patient-information-leaflets/pregnancy/pi-recurrent-and-late-miscarriage—tests-and-treatment-of-couples.pdf
- https://www.eshre.eu/Guidelines-and-Legal/Guidelines/Recurrent-pregnancy-loss.aspx
- https://www.asrm.org/topics/topics-index/miscarriage-or-recurrent-pregnancy-loss/


